Causes & Mechanisms
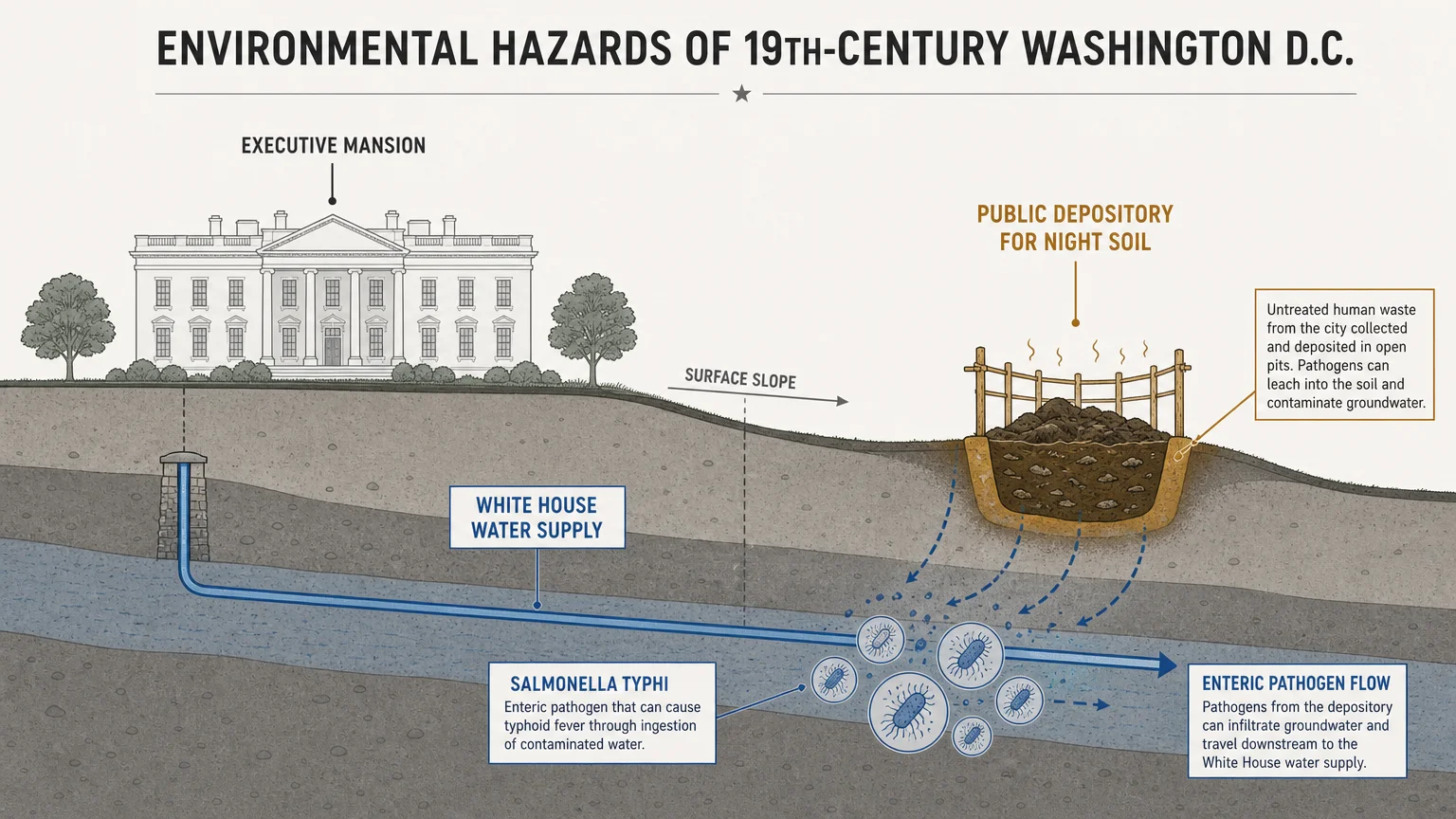
To understand the mechanics of these historical disasters, you must examine the specific medical science and security system failures that caused them. The first category of hazard involves environmental pathogens and systemic physiological failure. You can trace the deaths of William Henry Harrison in 1841 and Zachary Taylor in 1850 directly to the hazardous environmental conditions of nineteenth-century Washington, D.C. Early diagnoses blamed Harrison’s death on pneumonia and Taylor’s on generic gastroenteritis caused by consuming raw cherries and iced milk. However, modern epidemiologists point to a shared root cause: enteric pathogens. We define an enteric pathogen as a microscopic organism, such as Salmonella typhi, that infects the gastrointestinal tract. During the mid-nineteenth century, the White House water supply sat geographically downstream from a public depository for night soil—untreated human waste. This proximity created an acute environmental biological hazard, effectively pumping lethal bacteria directly into the executive mansion.
The death of James A. Garfield in 1881 presents a textbook case study in iatrogenic mortality, meaning death caused by medical examination or treatment. Garfield suffered a targeted ballistic trauma—a physical injury caused by a projectile—when an assassin shot him in the back. The bullet itself missed vital organs and safely encapsulated in his tissue. However, medical professionals of the era broadly rejected Joseph Lister’s emerging germ theory. Over several weeks, physicians repeatedly probed the wound channel with unwashed, bare fingers. This gross violation of sterile technique introduced severe external bacteria into Garfield’s bloodstream. He ultimately died from septicemia, a life-threatening systemic response to infection where bacteria aggressively multiply in the blood, leading to multi-organ failure. You can view his death as a catastrophic failure of medical protocol rather than a strictly fatal wound.
Cardiovascular disease serves as the fatal mechanism for Warren G. Harding and Franklin D. Roosevelt. In the early twentieth century, doctors lacked the diagnostic tools and pharmaceutical interventions to manage severe hypertension and atherosclerosis. Roosevelt’s death demonstrates this vividly. By early 1945, FDR’s blood pressure routinely spiked to catastrophic levels, frequently recording above 200/120 mmHg. On the day of his death, his physiological systems suffered a massive cerebral hemorrhage. You can define a cerebral hemorrhage as a ruptured blood vessel inside the brain, which immediately destroys local tissue and halts central nervous system functions. The medical infrastructure of the era possessed absolutely no mechanism to reverse or mitigate this acute vascular disaster once it began.
The assassinations of Abraham Lincoln, William McKinley, and John F. Kennedy expose the severe shortcomings in early threat intelligence and physical security architectures. In all three instances, threat actors managed to breach the immediate physical perimeter of the president to deliver fatal ballistic trauma. Security details in 1865 and 1901 operated without modern magnetometer screening, specialized crowd surveillance, or spatial distancing protocols. By 1963, despite the professionalization of the Secret Service, systemic intelligence-sharing failures allowed a known threat actor to exploit an unfortified, elevated vantage point above an open-top vehicle. The resulting high-velocity ballistic impacts destroyed vital neurological and vascular systems instantly, demonstrating how a localized security failure results in an immediate national crisis.



















1 thought on “8 Presidential Deaths That Changed America”
This was a very well-written and researched article. I thought I knew this information already. I did not. I learned something today. Some of the presidents I’m familiar with, were actually beneficiaries of the 25th Amendment.